Licensing
Product Case Studies
Canker sores are ulcers that affect the mucous membranes inside the mouth that are usually developed on the inner cheeks, gums or lips and, occasionally, the tongue. They may occur singularly then we use the term Aphthous stomatitis lesions or in groups then we use the term Recurrent aphthous stomatitis (RAS).The major difference between them is the frequency or severity of the outbreak(s). There are three forms:
- minor, flat small, lasting 5-10 days,
- major, large (lasting 2-3 weeks);
- raised borders.
Before it becomes visible, the canker sore may produce a tingling or burning sensation. After 6-24 hours, the ulcer appears as a small, round depression 0.3 to 0.6 mm in diameter, surrounded by a reddened area of inflammation.
The center is often grayish-white, due to a layer of dead cells - but underneath this layer, the tissue is extremely red and raw looking. A minor canker sore is most painful during the first 3-4 days. The discomfort gradually diminishes and the sore heals in 10-14 days, usually without scarring. Canker sores may recur with variable frequency depending on, various factors.
Canker sores are often studied, but a largely misunderstood phenomena. It has been termed the most common oral mucosal disease known to human beings, p lague the lives of millions. While for some these small oral ulcerations present only a minor nuisance, for others, canker sores (mouth ulcers) make life nearly unbearable. In fact, canker sores affecting nearly 20% of the population.
It has been noted that oral trauma may precipitate the development of RAS in certain susceptible individuals (Woo et al, 1996). In a study of 128 RAS patients, 20 claimed a previous traumatic incident. The trauma required to stimulate canker sores production could include biting the mucosa, tooth brushing, dental injection or certain sharp foods (Rees et al 1996). Trauma is not an associated factor in all patients, but it should be considered precipitating factor. Numerous researchers have attempted to explain the cause of RAS by way of some viral or bacterial factor. Several strains of streptococci and viruses have been suggested as a cause, but to date, have not been proven conclusively (Ship J et al, 1996). There was no evidence to support the theory of viruses as a cause of RAS based upon cultures, antibody titers, cytology or electron microscopy (Vincent SD et al, 1992). Genetic factors seem to play one of the biggest roles in patients with RAS. The presence of RAS is increased in patients with a positive family history (Vincent SD et al, 1992). Approximately 50% of first-degree relatives of patients with RAS are also RAS sufferers. Patients with a family history tend to develop RAS at an earlier age, and more severely than those patients with no positive family history (Woo et al, 1996). Vitamin deficiencies have frequently been noted in RAS patients. Deficiencies in vitamins B1, B2, B6, B12, folic acid, iron or zinc have been shown to occur twice as often in RAS patients versus control groups. Approximately 20% of RAS patients studied in various trials have deficiencies in vitamins of the above list (Rees at al, 1996). In general, spicy foods, acidic fruit juices, and carbonated drinks, are not recommended, although relationship between nutritional deficiencies and canker sores is controversial.
Stress was also mentioned as a factor of RAS development although it is controversial as well. Pedersen et al (1989) found no association between psychological life stress and recurrences of RAU , and concluded that more standardized circumstances are needed if any such association should be demonstrated.
There is nothing yet, that stops canker sores from recurring, but there are simple rules which may diminish the symptoms and relieve the discomfort. Treatment may reduce the infection in the area, during the 3-4 days when the sores are likely to be painful. Home version antiseptic, like teaspoon of salt and baking soda in a cup of warm water , should be used as rinses or gargles four times a day. Because this treatment option is so inexpensive it is worth trying. It is also helpful to avoid acidic foods and Certain Preservatives that may irritate the sores. It is advisable to avoid using any product containing Sodium Lauryl Sulphate (SLS),as well. Barkvoll and Brokstad (Barkwall et al, 1989) revealed a 60-70% reduction in the number of canker sores in patients who used SLS free toothpaste during the 3month test period. Not vitamins nor special foods help the condition unless a specific deficiency exists. Although stress is a controversial factor in canker sores and affects their intensity and severity, tranquilizers seem to give little relief.
Corticosteroids act by treating the inflammation associated with canker sores. These corticosteroids in gel or cream form are usually applied three to four times a day. Muzio conclude that topical application of clobetasol in an adhesive denture paste is an effective drug for symptomatic oral vesiculo-erosive and/or ulcerative lesions(Muzio et al 2001). Examples for corticosteroids found in the market across the world are 0.5% Lidex (Fluocinonide) and Triamcinolone acetonide, commonly known as Kenalog in orabase.
Analgesic (pain relieving) compounds are very common in the treatment of RAS and canker sores. The active ingredients often found in these compounds include Benzocaine ,Dibucaine or Diphenhydramine HCL. In addition to providing pain relief, several analgesic compounds form an adhesive film over the canker sore which blocks exposed sensory nerve in the canker sore. It also protects the sore from mouth acids and foods. Yamamura reported that a water-soluble three-layered oral mucosa-adhesive film made from hydroxypropyl cellulose containing dibucaine (0.25 mg of drug/cm(2)),induced Pain relief lasted for 2-5 h after application of the dibucaine film (Yamamura et al, 1999).
Anti-Microbial agent (anti-bacterial) in mouthwashes have been shown to be very beneficial in reducing canker sore pain. studies have shown that medicated mouthwashes containing chlorhexidine gluconate (Peridex) are effective in helping canker sore sufferers. Topical medications, such as antimicrobial mouthwashes, can achieve the primary goals but have not been shown to alter recurrence or remission rates .( Barrons RW et al).An interesting example for such a drug is ORA5 ,a topical antibacterial agent. It comprised primarily of copper sulfate which reduces mouth sore pain and iodine which acts as an antibacterial and anti viral agent. This medication creates a covering over the tender tissue and exposed sensory nerves of the open sore. When no nerve endings are exposed, there is no pain. By covering these exposed nerve endings ORA5 acts like a natural band aid.
Dr. Hunter and Dr. Addy showed that chlorhexidine gluconate mouthwash used three times a day reduced the total number of ulcer days experienced by patients by approximately 20 percent (Hunter L et al).
Mouthwashes containing chlorhexidine gluconate, however, should only be used in patients who normally experience moderate to severe cases of canker sores as this mouthwash can stain teeth.Anti inflammatory agent are very effective as well. 5% Amlexanox oral paste (Aphthasol) was studied in four vehicle-controlled, randomized, double-blind, parallel group, multicenter, clinical studies involving 1335 subjects who had 1 to 3 aphthous ulcers less than 48 hours old at enrollment. Subjects applied study pastes directly to ulcers four times a day until ulcers healed or for the duration of the study, whichever occurred first. Ulcer size was measured by the investigator and pain was evaluated by the subject; the primary determinant of efficacy was the percentage of subjects with complete healing of ulcers and complete resolution of ulcer pain. The vehicle had marginal beneficial effects as would be expected from a covering material, but statistical significance over no treatment was inconsistent. However, these studies, both individually and collectively, clearly demonstrated in a highly significant and consistent manner that in comparison to both Vehicle and No Treatment 5% Amlexanox oral paste accelerates the resolution of pain and healing of aphthous ulcers (Khandwala A et al).
An issue of the Journal of the American Dental Association reported in 1994 on a patch containing an aloe vera derivative. The patch can be applied to canker sores. According to research at the Baylor College of Dentistry in Dallas, Texas, the patch containing the aloe vera derivative (acemannan hydrogel) reduced healing time as well as pain associated with the canker sores. The Acemannan patch has received FDA approval and is currently being sold as the Carrington Patch (Publication Types: News).
Aphthous stomatitis lesions (Canker sores ) are ulcers that affect the mucous membranes inside the mouth,usually on the inner cheeks, gums or lips and, occasionally, the tongue.
Aphthous stomatitis lesions are characterized by the development of painful, recurring necrotizing ulcerations of the oral mucosa ,either as solitary or multiple lesions (RAS).While for some, these small oral ulcerations present only a minor nuisance, for others, canker sores (mouth ulcers) make life nearly unbearable. Current treatments are palliative and focus on pain and inflammation reduction. It involves the use of mouth wash, avoidance of irritating food and drinks, and local treatment with ointments and tinctures.
This study reports on the development of a bioadhesive patch that sticks and blocks the ulcer while releasing bioactive agents, for reduce pain and inflammation.
Preparation of patches and release of active agent
The Bioactive patches loaded with essential oil were prepared by mixing the oil with the polymer powders and compress the powder into a disc . Single patch was attached to a bottom of 10 ml vial,followed by the addition of 4 ml buffer and 3 ml hexane. The vial was kept at 370C with constant stirring. Specimens of hexane were taken at each interval, until complete degradation occurred. The optical density (OD) of the releasing medium was determined by ultraviolet (UV) detection.
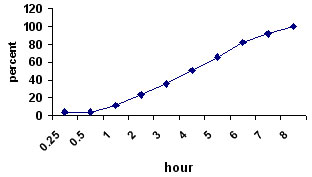
Release-time profile of active ingredients from patch in artificial saliva.
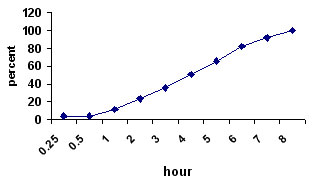
Accumulation time profile of active ingredients in artificial saliva.
Adherence to mucosal tissue
The adhesiveness of the patch when placed onto mucosal tissue was determined by using a tensiometeraim. The patch was stack onto the flat surface of the moving crimp of the tensiometer. Gingival tissue from cattle mouth was fixed onto a flat surface attached to the static crimp Both surfaces were connected for 10 to 300 seconds before measuring the adherence strength using Instron, model 4502.
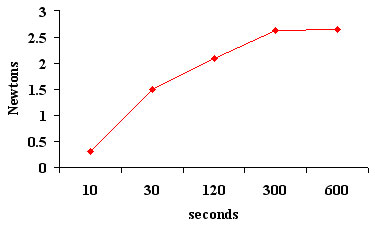
As long as the patches are being attached to the gingiva for at least 10 seconds, to produce tensile force of 0.32 N(32gr),the patches will remain on the gingiva. The maximum strength required to detached patches of the gingiva is 2.65 N (265gr).
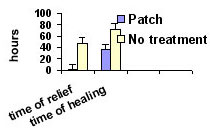
A total of 94 patients with a single, painful aphthous ulcer and 124 cases of RAS (with a frequency of once every month or more) were documented. The efficacy of treatment with the patches, as well as a patient satisfaction were documented.Time for healing was estimate by a specialized dentist.
Aphthous stomatitis RAS
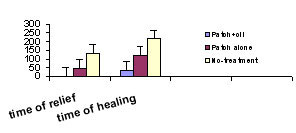
Local delivery of bioactive herbal medications for treating oral ulcers using a bioadhesive patch was found effective in humans.
The bioadhesive patch was effective in shielding the ulcerative wound from irritating factors in the oral cavity.
The patch locally deliver a bioactive agent for extended period and consequently is highly effective in reducing pain and time of complete recovery.
Canker Sores: What are They and What Can You Do About Them? general overview of mouth ulcer.
http://www.familydoctor.org/handouts/613.html
Fever Blisters and Canker Sores
describes the symptoms, treatment, and differences between these two common disorders of the mouth. From the National Institutes of Health.
http://www.pueblo.gsa.gov/cic_text/health/fever-blister/fever-canker.html
MayoClinic.com: What Are Canker Sores?
describes symptoms, possible causes, treatment, and self care.
http://www.mayoclinic.com/invoke.cfm?id=DS00354
MEDLINEplus: Canker Sores
benign, open sores in the soft tissues of the mouth that are also known as aphthous ulcers.
http://www.nlm.nih.gov/medlineplus/ency/article/000998.htm
Mouth Ulcers
provides information, surveys, a message board, and more.
http://www.mouthulcers.org
The Difference Between a Canker Sore and a Cold Sore?
http://www.healthfinder.gov/docs/doc04185.htm
All about canker sores
http://icrc.bumc.bu.edu/view.asp?pageid=186